SR-17018 and Opioid Tolerance
How receptor desensitization, intracellular adaptation, biased agonism, and MOR signaling may shape opioid tolerance biology.
Opioid tolerance is one of the defining biological features of long-term opioid exposure.
Over time, repeated opioid use often produces diminishing effects, requiring progressively larger doses to achieve the same level of analgesia, intoxication, withdrawal suppression, or emotional relief.
This process contributes heavily to:
- dose escalation
- dependence progression
- overdose risk
- withdrawal severity
- fentanyl transition
- loss of functional stability
SR-17018 has entered scientific and harm reduction discussions because preclinical studies suggest it may interact with opioid tolerance differently than many classical opioids.
SR-17018 is not important simply because it activates the mu opioid receptor. It is important because it may activate that receptor differently.
What Is Opioid Tolerance?
Opioid tolerance occurs when repeated opioid exposure causes the nervous system to adapt to ongoing receptor activation. As these adaptations accumulate, the same opioid dose produces a weaker effect over time.
Tolerance is not merely psychological. It is a biological response involving receptor regulation, intracellular signaling changes, gene expression shifts, neurotransmitter adaptation, and broader nervous system compensation.
The body essentially attempts to restore equilibrium while opioids continue pushing the system in the opposite direction.
This is why someone who initially experienced strong effects from a small opioid dose may eventually require dramatically larger amounts to achieve similar effects.
The Mu Opioid Receptor and Adaptation
Most clinically important opioids exert their primary effects through the mu opioid receptor, commonly abbreviated MOR.
When opioids repeatedly activate MOR, the receptor system begins adapting in several ways:
- receptor desensitization
- receptor internalization
- β-arrestin recruitment
- intracellular signaling compensation
- cAMP pathway rebound
- broader neural circuit adaptation
These changes are part of why opioid tolerance develops.
Importantly, tolerance is not controlled by a single mechanism. It is a network-level adaptation process involving both receptor biology and larger nervous system changes.
Tolerance is essentially the nervous system learning how to function in the ongoing presence of opioid receptor activation.
cAMP Rebound and Dependence
One major component of opioid adaptation involves cyclic AMP, often abbreviated cAMP.
Acute opioid exposure suppresses cAMP signaling in many neurons. Over time, however, the nervous system compensates by upregulating cAMP-related pathways in an attempt to restore balance.
When opioids are removed suddenly, those compensatory systems become overactive.
This contributes to withdrawal symptoms such as:
- anxiety and sympathetic activation
- restlessness and agitation
- pain hypersensitivity
- gastrointestinal distress
- autonomic instability
Tolerance and withdrawal are therefore deeply connected. The same adaptations that reduce opioid responsiveness also help create dependence and withdrawal biology.
Biased Agonism and SR-17018
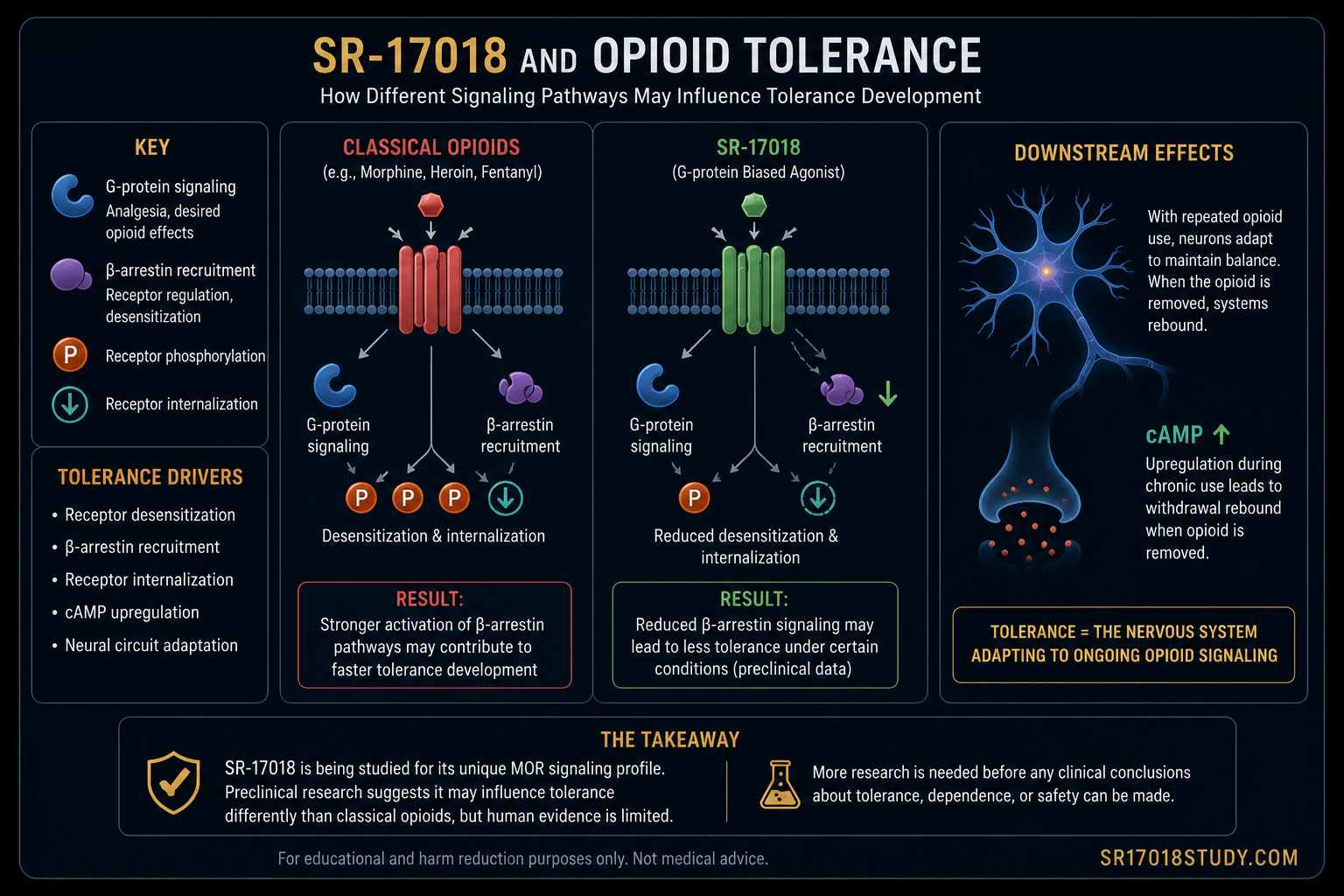
SR-17018 is often discussed in relation to biased agonism, a concept suggesting that different ligands can activate the same receptor while favoring different intracellular signaling pathways.
In opioid pharmacology, this discussion often focuses on:
- G-protein signaling
- β-arrestin recruitment
Preclinical studies suggest SR-17018 may strongly activate G-protein signaling while producing relatively reduced β-arrestin recruitment compared with many classical opioids.
This matters because β-arrestin recruitment has been studied as one contributor to receptor desensitization and adaptation processes associated with tolerance.
The central scientific question is whether changing opioid receptor signaling changes how tolerance develops.
Why SR-17018 Became Interesting in Tolerance Research
Some preclinical studies have suggested that SR-17018 produces unusual effects in opioid tolerance models. In certain experiments, SR-17018 appeared capable of reversing morphine tolerance or producing less tolerance under specific testing conditions.
These findings attracted major interest because opioid tolerance is one of the largest unsolved problems in pain management and addiction medicine.
If a compound could preserve useful opioid receptor effects while reducing tolerance escalation, it would represent a potentially important pharmacological advance.
However, the data are more complicated than internet discussions often suggest.
Other studies have shown that SR-17018 can still produce tolerance or dependence-related effects depending on:
- the experimental model
- the tissue type
- the assay used
- the dosing schedule
- the behavioral endpoint being measured
This is why responsible interpretation requires nuance rather than hype.
Why Animal Data Have Limits
Most SR-17018 tolerance research remains preclinical.
Animal models are extremely useful for studying receptor signaling and adaptation mechanisms, but they cannot fully capture the complexity of human opioid dependence.
Human tolerance is influenced by:
- fentanyl exposure
- polysubstance use
- stress physiology
- sleep disruption
- pain disorders
- psychiatric illness
- nutrition and endocrine status
- social instability
- product variability
A compound may behave differently in controlled laboratory settings than it does in real-world human environments.
That does not invalidate the mechanistic findings. It simply means the findings should be interpreted carefully.
Why Tolerance Matters in the Fentanyl Era
Modern fentanyl exposure has intensified the tolerance problem dramatically.
Many people develop extremely high opioid tolerance levels that make stabilization, induction, tapering, and withdrawal management far more difficult than during earlier heroin-dominated eras.
As tolerance escalates:
- overdose risk rises
- withdrawal severity increases
- daily functioning deteriorates
- financial instability worsens
- transition attempts become harder
This is one reason people have become interested in compounds that may interact with MOR signaling differently than classical opioids.
SR-17018 has entered that discussion because it may provide insight into whether opioid receptor signaling itself can be modified in a way that changes tolerance trajectories.
What SR-17018 Does NOT Prove
One of the biggest mistakes online discussions make is turning mechanistic interest into exaggerated clinical claims.
SR-17018 has not been proven to:
- eliminate tolerance
- prevent dependence
- replace methadone
- replace buprenorphine
- reverse addiction safely in humans
- provide guaranteed respiratory safety
Human data remain extremely limited.
Mechanism can generate scientific hypotheses. It does not automatically prove real-world safety or effectiveness.
The scientifically responsible position is not “SR-17018 solves opioid tolerance.” The responsible position is: “SR-17018 raises important mechanistic questions about how opioid tolerance develops.”
The Real Takeaway
Opioid tolerance is one of the central biological drivers of dependence, overdose risk, and the modern fentanyl crisis.
SR-17018 matters because it may challenge assumptions about how tolerance develops at the mu opioid receptor.
Its potential significance is not that it is “another opioid,” but that it may represent a different pattern of opioid receptor signaling and adaptation.
Whether that ultimately translates into meaningful human benefit remains unknown.
SR-17018 should be viewed neither as a miracle compound nor as meaningless internet hype. It should be viewed as a scientifically important research molecule whose relevance depends on careful evidence-building and honest pharmacological discussion.
Sources and Further Reading
- Grim TW et al. A G protein signaling-biased agonist at the μ-opioid receptor reverses morphine tolerance while preventing morphine withdrawal. PDF.
- Gillis A et al. Low intrinsic efficacy for G protein activation can explain improved side effect profiles of newer opioid agonists. Science Signaling.
- Fritzwanker S et al. SR-17018 stimulates atypical μ-opioid receptor phosphorylation and dephosphorylation. PMC.
- Pantouli F et al. Comparison of morphine, oxycodone and the biased MOR agonist SR-17018 in opioid tolerance and dependence models. ScienceDirect.
- National Institute on Drug Abuse. Medications for Opioid Use Disorder. NIDA.